Amodei's compressed century stops at deployment.
Dario Amodei's "Machines of Loving Grace" landed October 11, 2024. The argument: powerful AI compresses 50-100 years of biomedical progress into 5-10 years. The essay is the most-cited frontier-lab CEO healthcare-optimism document of the year. Two months later the discourse is still working through it.
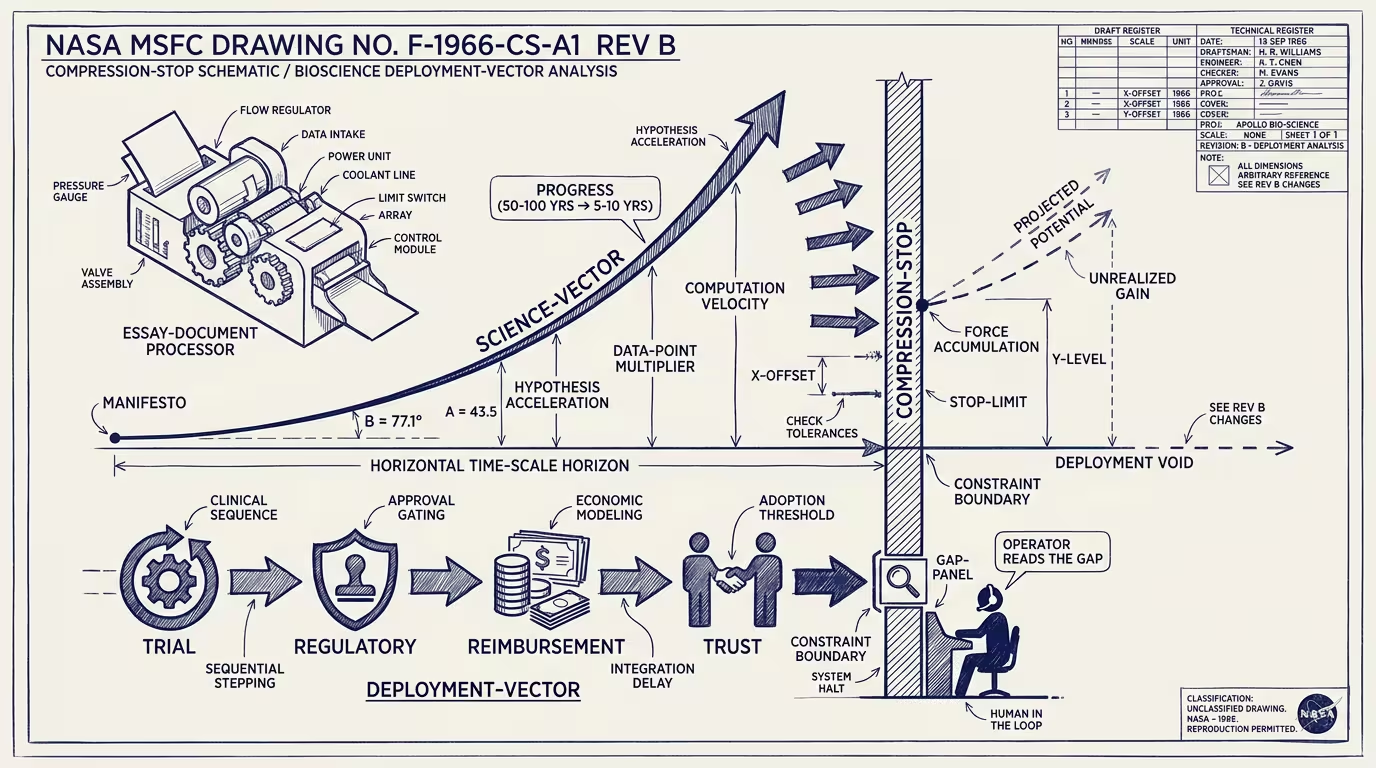
Read flat, the essay is right on the science vector and silent on the deployment vector. _The compression Amodei describes stops at deployment._
The science vector is what Anthropic's models can accelerate. Biology compresses on the AI-capability curve because the rate-limiting step in modern biology is increasingly hypothesis-generation, experiment-design, and data-pattern-recognition — three tasks AI is structurally good at. The 100-years-in-a-decade projection, on the science vector, is plausible. Plausible enough that Amodei's specific examples (mental health interventions, neurodegeneration, oncology) cite real mechanism-of-action improvements that AI is materially accelerating.
The deployment vector is what gets the compression to the patient. _It does not run on the model-capability curve._
The deployment vector runs on five layers, none of which the Amodei essay engages with at substance.
Reimbursement. A new therapy reaches the patient through a payer that pays for it. CMS coverage decisions take 24-48 months from FDA approval to consistent payer coverage. Private payers follow CMS on a 6-12 month lag. The therapy that exists technically in 2026 reaches scale in 2030.
Liability. The clinician carries malpractice exposure for novel AI-assisted treatments. The malpractice insurer needs actuarial data, which does not exist for novel categories until the first wave of cases produces claims and settlements. The lag is 5-7 years.
Clinical workflow. A new diagnostic that requires new test ordering, new sample collection, new EHR fields, new physician review compounds at 18-24 months per workflow change. AI does not compress that timeline.
Physician trust. Clinical adoption runs on peer-recommendation and journal-publication mechanisms calibrated to social-proof timelines that are decades old. The 100-year-in-a-decade compression requires physician knowledge to absorb faster than the published-evidence-base accumulates. That is not how clinical practice works.
Regulatory pacing. FDA review timelines, while compressing, do not run on the model-capability curve. The agency's 2024-2025 investment in AI-specific review processes accelerates the timeline by some, not by 10x.
The five together are the deployment-layer gap. The technical layer compresses. The deployment layer does not. The compression at the technical layer produces a backlog at the deployment layer, and the backlog is where the actual patient-outcome story lives for the next decade.
The cohort-cost of that gap is paid by the patient. A novel cancer therapy that exists technically in 2026 but is not reimbursed until 2030 is a therapy available to private-pay patients with launch-price flexibility for a four-year window, and unavailable to the cohort that needs the reimbursement decision. Some of that cohort dies waiting. The Amodei timeline does not name this. The gap is, of course, where the operating economics of AI's clinical impact have to be modeled.
The read that survives is that Amodei's essay is correct about what is upstream of the deployment layer and silent about what is at the deployment layer. The trade press read the essay as universally optimistic; the part that holds should be partial. _The compression is real. The compression stops at deployment._
The operator-class question worth asking: which side of this gap is the operator's product on? The healthtech operator whose product depends on the deployment layer working faster (pre-clinical AI tools that ride downstream regulatory acceleration, reimbursement-acceleration platforms, real-world-evidence registries that compress liability timelines) is on the side that captures the next-decade outcome. The operator whose product depends only on the technical layer compressing is the operator whose 2027 deployment is impressive in the demo and inert in the field.
Amodei is right about the science. He is silent on the part the operator should be building against. The compression stops at deployment. The operators who fill that silence are the operators whose 2030 outcomes match the essay's projection. The rest, in operating practice, watch the projection arrive late, on a curve the essay didn't model.
—TJ