Canada legislated in 2024 what the US did in 2016. Here is what that decade of lag costs.
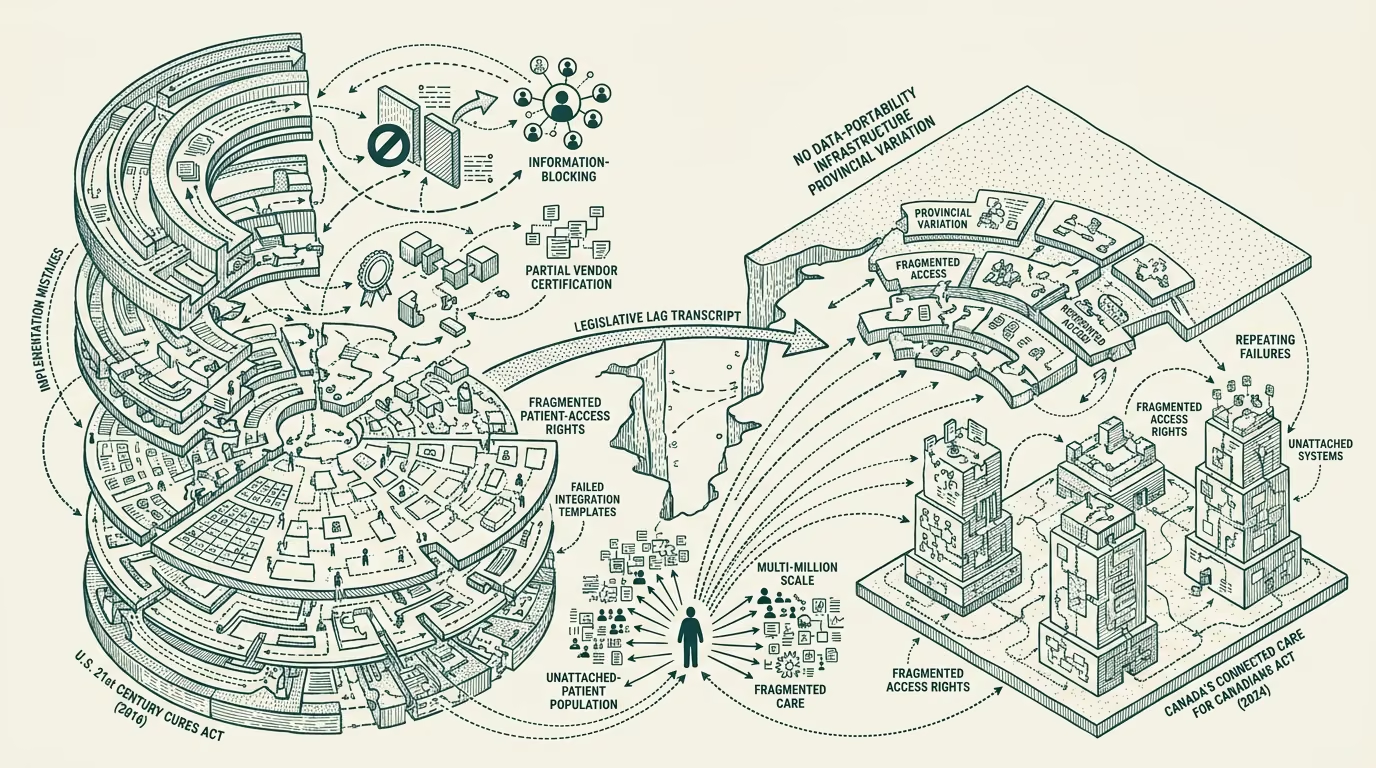
Canada's Connected Care for Canadians Act, Bill C-72, received Royal Assent in June 2024. The bill creates a federal framework for health-data interoperability across Canadian provinces, with provisions for data-portability, patient-access rights, vendor-side certification requirements, and information-blocking prohibitions. The structural shape of the legislation is recognizable to anyone who has worked on the U.S. equivalent: it is the Canadian version of the 21st Century Cures Act of 2016, with the major provisions arriving roughly eight years after the U.S. equivalent did.
The decade of lag is partly a feature and partly a cost. The feature side is that Canadian implementation can learn from the U.S. trajectory's mistakes, of which there were several substantial ones. The cost side is that the Canadian healthcare system has been operating for a decade without the data-portability infrastructure that the legislation is finally now requiring. The provincial-level variation in Canadian healthcare, the unattached-patient population running at multi-million scale, the chronic family-doctor shortage: all of these have been compounded by the absence of the data-portability infrastructure the bill now mandates.
This essay walks the legislative parallel, the U.S. implementation trajectory's mistakes through 2016-2024, which mistakes the Canadian implementation is structurally on track to repeat, and what Canadian operators reading the U.S. transcript should do differently.
The legislative parallel
The 2016 21st Century Cures Act in the U.S. established a federal framework for health-data interoperability with several structurally similar provisions to Bill C-72: information-blocking prohibitions on EHR vendors and health systems, patient-access rights to their own clinical data through APIs, vendor-certification requirements through ONC, and federal authority over the certification-and-enforcement infrastructure. The implementation work happened over the subsequent eight years, with the major rules (the 2020 ONC Cures Act Final Rule, the various enforcement guidance documents, the TEFCA-and-QHIN buildout) shipping in stages.
Bill C-72 establishes a structurally similar framework at the Canadian federal level, with the implementation timeline still ahead and the implementation rules still to be drafted. The shape of the Canadian implementation work over the next 5-7 years will look like the U.S. implementation work over 2016-2024. The work is real, the timelines are long, and the implementation choices the Canadian regulators make will determine whether the legislation produces the data-portability outcomes it is meant to produce or whether it gets blocked by the same structural barriers that have constrained the U.S. equivalent.
The U.S. trajectory's implementation mistakes
The U.S. implementation between 2016 and 2024 made several mistakes that the Canadian implementation can learn from.
The first mistake was the long lag between the legislative authorization and the operational rules. The Cures Act passed in 2016, the ONC Cures Act Final Rule was published in 2020, the information-blocking enforcement provisions came online progressively through 2021-2023, and meaningful enforcement actions are still rare in 2024. The four-to-eight-year gap between the legislative intent and the operational consequence allowed the regulated parties (EHR vendors, health systems) to defer the structural changes the legislation required, with the result that the operational state in 2024 is closer to the 2018 baseline than the 2016 legislative ambition implied.
The second mistake was the under-investment in the certification-and-enforcement infrastructure. ONC has been chronically under-resourced relative to the scope of the regulatory work the Cures Act assigned to it. The certification body (ONC's Health IT Certification Program) processes a substantial volume of EHR vendor certifications, but the enforcement-and-audit infrastructure for the broader information-blocking rule has been thin enough that compliance has been mostly voluntary in practice. The under-investment slowed the operational rollout meaningfully.
The third mistake was the late attention to the patient-mediated access flow. The Cures Act included strong patient-access rights from the legislative text, but the implementation through 2020-2022 prioritized the institutional-to-institutional data flow (provider-to-provider, payer-to-provider) over the patient-to-app flow that the patient-access rights were meant to enable. The patient-mediated flow has caught up since 2022, with the Apple Health Records integration, the major patient-portal-to-app workflows, and the consumer-app ecosystem maturing. The earlier prioritization would have produced the patient-side benefits faster.
The fourth mistake was the under-specification of the vendor-side technical-and-contractual requirements. The Cures Act left substantial latitude to ONC and to the EHR vendors on what the technical-and-contractual posture should look like, with the result that the practical implementation has been negotiated bilaterally between the EHR vendors and their health-system customers, with substantial variation across the resulting integrations. Tighter specification at the rule-making stage would have produced more consistent operational outcomes.
Which mistakes Canada is structurally on track to repeat
Reading the Canadian implementation environment against the U.S. trajectory, several mistakes are structurally on track to repeat.
The lag between Bill C-72's June 2024 passage and the operational rules is structurally similar to the U.S. timeline. The provincial-federal coordination work in Canada is more complex than the federal-state coordination in the U.S. because provincial health systems are constitutionally independent, with the result that the operational rule-making timeline could be longer rather than shorter than the U.S. equivalent. Canadian operators planning against the legislation should expect the operational consequences to ramp through 2026-2030 rather than landing in 2025.
The certification-and-enforcement infrastructure question is structurally similar. Health Canada and the related federal regulatory bodies do not currently have the certification-and-enforcement capacity that ONC has built out (with all of ONC's limitations). Building that capacity requires multi-year investment that the federal budget has not yet committed to. The operational enforcement of Bill C-72 is likely to be thin in the early years, with the regulated parties having latitude to defer the structural changes.
The patient-mediated access flow is the area where Canada has the clearest opportunity to do better than the U.S. trajectory, because the Canadian implementation can learn from the U.S. lesson and prioritize the patient-mediated infrastructure earlier. Whether the implementation actually does so will depend on the political-and-bureaucratic priorities at the rule-making stage, and the early signals are mixed.
The vendor-side technical-and-contractual specification is the area where the Canadian implementation has the option to be tighter than the U.S. equivalent. The Canadian regulators can specify the technical requirements more precisely, the contractual terms more explicitly, and the audit-and-attribution infrastructure more rigorously than the U.S. rules did. Whether they will is uncertain.
What Canadian operators should do differently
For operators working in Canadian health-tech, the operator-class advice is to read the U.S. transcript carefully and build for the version of the implementation that does not repeat the U.S. mistakes.
The practical version of this advice is to invest in the patient-mediated infrastructure now, not later, because the patient-mediated flow is where the U.S. lag was most visible and the Canadian opportunity to leapfrog is largest. The patient-portal and patient-app ecosystem in Canada is structurally underbuilt relative to the U.S., and the operators who build patient-mediated infrastructure that fits the Bill C-72 framework will be in position to capture the operational returns the legislation is meant to produce.
The second practical advice is to pressure the federal-and-provincial regulatory work toward tighter technical-and-contractual specification, drawing on the U.S. lessons that under-specification produces variable operational outcomes. The operator-grade voice in the rule-making process is meaningful, and operators advocating for tighter rules will produce a more usable operational framework than the bilateral-negotiation approach the U.S. version drifted toward.
The third practical advice is to plan against the slower-than-the-legislation-implies operational rollout, because the certification-and-enforcement capacity will lag, and the regulated parties will defer. Operators who plan against the 2025-2026 timeline the legislation might imply will be disappointed; operators who plan against the 2027-2030 ramp will be right.
Canada legislated in 2024 what the U.S. did in 2016. The decade of lag is a fact. The lessons from the U.S. trajectory are available. The Canadian operators who read the transcript carefully will produce better implementation outcomes than the U.S. trajectory did, and the operators who do not read it will repeat the same mistakes on a Canadian timeline. The transcript is not subtle. The reading is the work.
—TJ