The national Canadian primary care crisis is quantified. The 6 million number changes the political calculus.
The OurCare initiative's national survey results in January 2025, with the Health Standards Organization endorsement, confirmed approximately 6.5 million Canadians without primary-care attachment. The number is the largest publicly-reported estimate produced through a methodology that the federal-and-provincial public-health establishment has accepted as credible. The previous estimates ran in the 4-5 million range across various regional and methodologically-different surveys, with the national-level number being implicit rather than explicit. The 6.5 million figure is the explicit national number, and it changes the political calculus in ways the earlier regional estimates did not.
The durable read on the trajectory has been visible to operators working in the Canadian primary-care space for several years. The marketplace-and-routing-layer mechanism that would address most of the gap is technically available, has been demonstrated at smaller scales, and is politically blocked at the financing-and-incentive layer. The 6.5 million number forces the political calculus on the financing question because the alternative scenarios (continued growth in the unattached population, continued migration to ED-and-walk-in for primary-care issues, continued physician-burnout from the over-stressed remaining attached-care infrastructure) are progressively untenable.
This essay walks the number, what it changes about the political calculus, the routing-layer financing question that has been the actual blocker, and what the durable read should be.
What the 6.5 million number actually means
The 6.5 million figure represents Canadians who do not have a regular family doctor or primary-care nurse practitioner they can access for non-urgent clinical issues. The methodological details matter. The number includes some subset of patients who have access to a community health centre or a clinic-based primary-care relationship that is structurally weaker than a traditional family-doctor attachment. The number includes a much larger subset of patients who have no consistent primary-care relationship at all and route their care through emergency departments, walk-in clinics, virtual-care services, and the various other ad-hoc channels that the Canadian system has been progressively absorbing the unattached-care load through.
The 6.5 million represents roughly 17 percent of the Canadian population. The rate is not evenly distributed. Some provinces (Quebec, Atlantic provinces) have rates closer to 25 percent. Some provinces (Ontario, BC) have rates closer to 12-15 percent. The age-and-demographic distribution is similarly uneven, with younger and lower-income populations having disproportionate exposure.
The trajectory through 2025-2027, on the current policy trajectory, projects continued growth past 7 million by 2026 and toward 8 million by 2027 absent meaningful intervention. The numbers are the kind of numbers that political accountability mechanisms eventually act on, even when the political-and-bureaucratic resistance to action has been substantial.
What changes about the political calculus
The political calculus on Canadian primary-care reform has been blocked through 2018-2024 by several reinforcing factors: the provincial-federal jurisdictional dispute over health-care delivery, the physician-and-college lobbying against scope-of-practice reforms that would expand non-physician primary-care capacity, the funding-formula complexity that makes the financing of new models politically costly, and the broader political-class inertia on a file that does not produce visible electoral consequence at the speed political timelines reward.
The 6.5 million number changes several of these factors.
The number is large enough to produce visible electoral consequence on a faster timeline than the political-class had been pricing in. Politicians whose constituents include unattached patients (which, at 17 percent of the population, includes meaningful fractions of every electoral riding) face direct accountability that the smaller previous numbers did not produce. The accountability is uneven across riding-shapes but is rising.
The number also produces media-and-trade-press coverage at sustained intensity that the earlier numbers did not. The crisis framing that the press carried through the second half of 2024 and into 2025 has shifted from regional-and-occasional to national-and-sustained, with the consequence that the political-class cannot defer engagement on the file as easily.
The number also produces operator-class organizing. Healthcare professional organizations, patient-advocacy groups, and the various policy-class entities engaging with the primary-care question have aligned on the 6.5 million as the working number, with the alignment producing more coordinated political pressure than the previous fragmented advocacy could.
The routing-layer financing question
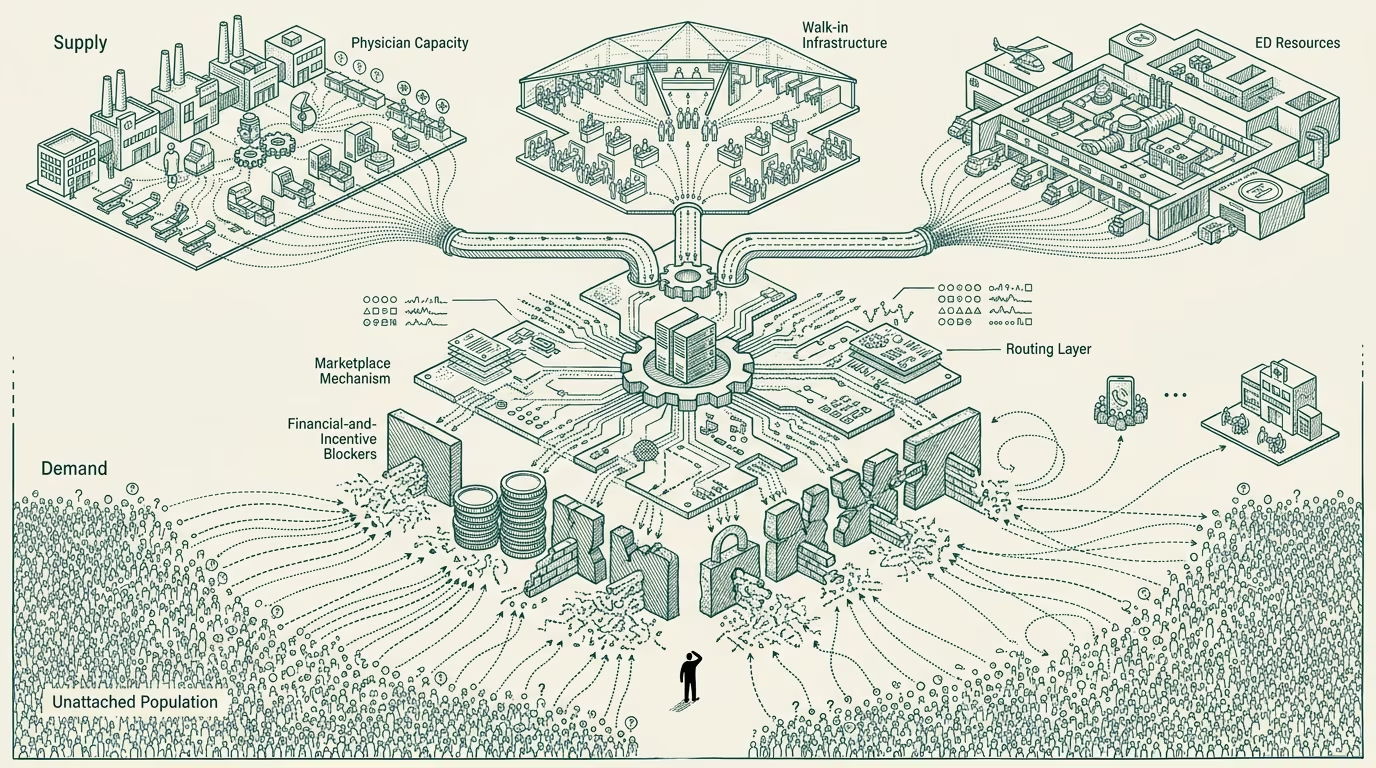
The technically-available solution to most of the unattached-patient gap is the routing-layer infrastructure discussed elsewhere: centralized or regionally-coordinated patient-attachment registries, team-based-care configuration,AI-augmented patient-routing tools, and the broader matching infrastructure that connects unattached patients to practices with available capacity.
The financing question is what blocks deployment. The provincial governments fund the existing physician-payment system (mostly fee-for-service, with some capitation in selected programs). The federal government provides transfer payments to the provinces with general health-funding earmarks. Neither structure has dedicated funding for the routing-layer infrastructure. Building the infrastructure requires a financing mechanism that does not currently exist, which means it requires political will to create one.
The routing-layer infrastructure cost is structurally smaller than the supply-expansion alternative cost. The political-and-bureaucratic difficulty of building the financing mechanism, however, is meaningful. The various proposals through 2024-2025 (federal-and-provincial cost-sharing programs, dedicated transfer payments tied to routing-infrastructure deployment, provincial-level innovation funds, the various patient-attachment initiatives that several provinces have been running) have been moving slowly and the cumulative deployment has been small relative to the gap.
The 6.5 million number creates the political pressure to accelerate the financing-mechanism work. The pressure is necessary but not sufficient. The mechanism still has to be built, and the political-class with the authority to build it has to commit the time-and-capital to the work.
What the operator class should take from this
For Canadian healthcare operators, the durable read is that the political calculus around routing-layer infrastructure is shifting toward action, with the 6.5 million number being the visible inflection point. The 24-36 month window for building products, services, and infrastructure that align with the routing-layer trajectory is open and active. Operators positioning their products as solutions to the primary-care attachment problem have a stronger market environment than they have had in any prior period.
For Canadian provincial health ministries, the durable read is that the political-cover for routing-layer investment is now substantial. Provincial-level innovation funds, attachment-program investments, and the broader routing-infrastructure deployment can be pursued with less political risk than was true in 2023-2024.
For federal-level engagement, the read is that the political pressure on a national-level financing mechanism is rising, with the corresponding opportunity for the federal government to take a coordinated leadership role on the file. The political-cover for federal action is substantial, and the inaction option is producing visible political cost.
The 6.5 million number is the political-economy-changing fact. The marketplace-and-routing-layer mechanism that would address most of the gap is available. The financing question is the bottleneck. The political pressure is now sufficient to make the financing question the active political work rather than the deferred political work it has been through the prior decade. The next 24-36 months will produce visible movement on this file, in directions the operator-tier running infrastructure-and-products in the space has been advocating for. The work is now political; the technical work is, comparatively, the easier part.
—TJ